We start with a one-on-one consultation to understand your needs, concerns, and goals.
2
Treatment Plan
Based on your consultation, we design a tailored treatment plan built around your lifestyle, budget, and expected results.
3
Ongoing Support
We provide continuous support, follow-ups, and progress tracking to ensure you’re improving comfortably and achieving long-term results.
Technology and Expertise
Technology We Use
Purpose-driven systems selected to enhance accuracy, comfort, and care.
iCAT 3D CBCT
A full 3D view of your teeth, jaw, and airway in one quick scan. Gives your orthodontist ultra-precise detail for safer, smarter treatment planning. Reduces guesswork so every movement is intentional. It’s basically the blueprint behind your best smile.
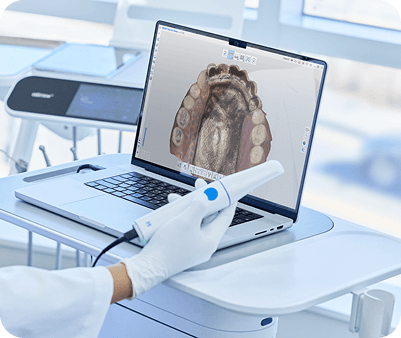
MediT Scanner
A fast, super-accurate digital scanner that replaces messy impressions. Captures every contour of your teeth in seconds. More comfort for you, more precision for your treatment. Your aligners and appliances fit better because the data is honestly next-level.
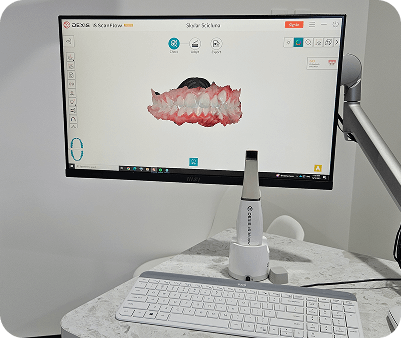
Dexis Scanner
High-resolution imaging that picks up tiny details regular scans miss. Ideal for accurate diagnostics and treatment monitoring. Smooth, comfortable scanning experience with real-time visuals. Helps your orthodontisYoat Wire Bender A digital wire-bending systt make confident, data-backed decisions.
SprintRay 3D Printer
Allows your clinic to print custom appliances, models, and trays in-house. Cuts down waiting time and improves treatment efficiency. Every print is sharp, accurate, and built to fit your smile. Faster turnaround, cleaner workflow, happier patients.
Autoclaves
Hospital-grade sterilization for every instrument used in your treatment. Kills bacteria, viruses, and spores within minutes. Ensures every visit is hygienic and safe, no compromises. Your health stays protected at every step.
Grin
A remote monitoring system that lets your orthodontist track progress digitally. You send smile scans from home; your doctor reviews and guides you. Fewer in-clinic visits, more convenience, same expert oversight. Perfect for busy schedules without slowing down your treatment.
Yoat Wire Bender
Yoat wire-bending technology allows for precise, computer-guided fabrication of orthodontic wires. By translating digital treatment plans into accurately bent wires, it supports controlled tooth movement and greater consistency throughout treatment. This technology enhances efficiency, predictability, and clinical precision while reducing manual variability.